In early 2026, the FDA began to shift how drug development unfolds. In March 2026, the agency announced steps to implement real-time clinical trial models, allowing regulators to observe predefined safety and efficacy signals as trials progress rather than waiting for completed data packages. At the same time, FDA leadership publicly advocated for one adequate and well-controlled pivotal trial, supported by confirmatory evidence, as the default pathway for approval, moving away from the historical two-trial requirement. Together, these changes point toward more immediate proof, faster feedback, and more continuous learning throughout the development lifecycle.
For early‑stage organizations, the implication is not simply speed but compression: timelines shorten, but more importantly, decision cycles that once occurred sequentially now overlap and must be managed in parallel. Choices about endpoints, manufacturing, and evidence strategy, traditionally addressed in distinct phases, now converge. This dynamic reflects a shift from sequential to concurrent, interdependent decision-making, in which trade-offs must be managed in real time with limited opportunity for course correction. Consequential risks, including endpoint misalignment, population selection errors, and manufacturing pathway commitments, surface sooner in the development lifecycle, often before full validation is possible.
Success in this environment increasingly depends on leadership judgment: the ability of CEOs, boards, and leadership teams to interpret emerging signals, such as early clinical data, safety observations, and competitive intelligence, and act on them before complete certainty arrives. Traditional milestones still exist, but they no longer provide the buffer they once did. As a result, leaders’ judgment is tested under conditions of reduced optionality, with fewer opportunities to defer, correct, or recover once commitments are made.
Tolerance for Delay Is Disappearing
Even as expectations shift toward earlier development decisions, the industry is taking longer to generate human evidence. Trial startup and early‑phase timelines are lengthening, driven less by statutory FDA review timelines than by operational friction across contracting processes, institutional review workflows, and fragmented infrastructure. FDA leadership and industry commentary point specifically to contracting delays, IRB variability, and pre‑IND processes as material bottlenecks in early‑phase activation (Becraft, 2026).
These dynamics accumulate across the system and intensify demands on early stage organizations to accelerate trial activation and reach interpretable human
data faster. These companies carry risk longer, often with limited margin for error, while capital decisions wait for clearer evidence. Simultaneously, global competition intensifies. Other geographies streamline early clinical development, and accelerated trial initiation increases the premium on reaching interpretable human signals rapidly (Becraft, 2026).
In combination, these forces reduce tolerance for delay and create conditions for regulatory approaches that prioritize initial clarity over later correction.
Earlier Proof, Not Faster Process
Recent FDA actions are responses to these structural pressures. While often discussed as discrete policy changes, these actions point to a broader shift toward front-loaded and more continuous evidence generation.
The agency is beginning to test real‑time clinical trial models in which safety signals and endpoints stream to regulators as trials progress. Instead of waiting for completed data packages, FDA scientists can observe predefined signals in real time, reducing the lag between data generation and regulatory insight (FDA, 2026).
Alongside this, FDA leadership has stated that one adequate and well‑controlled pivotal trial, supported by confirmatory evidence, should serve as the default for approval. This shifts the emphasis from repeating late‑stage studies to ensuring that trial design, endpoints, and execution are right the first time (Prasad and Makary, 2026).
These developments do not represent deregulation but rather a rebalancing: less reliance on sequential staging and more focus on establishing decision‑quality evidence earlier in the process through optimized rigor in clinical trial design.
However, compression also introduces new risks. When critical choices occur closer together with fewer opportunities to revisit assumptions, acting on emerging signals, such as early clinical data, interim safety observations, pharmacokinetic profiles, and biomarker responses, can increase the likelihood of responding to incomplete or transient information. Decisions on endpoints, populations, or manufacturing pathways can lock in assumptions before full validation. As optionality narrows, the cost of misalignment rises as decisions become binding earlier. The challenge is not speed itself, but ensuring that the quality of early identification, interpretation, and action rises materially to match compressed timelines. Organizations that lack this capability risk moving quickly in the wrong direction. This is not a regulatory risk; it is a leadership capability risk.
Leadership Moves Upstream
If the system is under pressure and the regulatory model is shifting, the implications ultimately fall on leadership. Decisions that once unfolded sequentially now overlap, and the scope of leadership capabilities required expands significantly and arrives much earlier in the development cycle. As we noted in our prior work on Milestone Leadership (WittKieffer, 2026), different stages of development traditionally demanded different leadership capabilities. When milestones compress, the full spectrum of capabilities, from scientific judgment to regulatory strategy, commercial insight, and operational execution, must be present and integrated from the outset, rather than accumulating progressively.
Trial design becomes a leadership‑level decision. When a single pivotal trial becomes the default, endpoint selection becomes a value‑defining decision, not a Phase 3 detail. Patient population, control arms, and statistical assumptions no longer sit within a purely technical domain they define enterprise risk. Boards and CEOs must engage sooner because misjudgments leave fewer opportunities to recover.
Execution risk concentrates earlier. Faster pathways do not eliminate risk; they intensify it and pull it forward. Decision latency, unclear ownership, and delayed escalation surface more quickly and with greater consequences. The challenge is not only scientific uncertainty; it is organizational readiness to respond to emerging data with discipline and speed.
Manufacturing and evidence strategy move upstream. Shortened development cycles pull forward decisions traditionally treated as downstream. Manufacturing readiness, CMO selection, and scale commitments must align with accelerated clinical timelines. At the same time, evidence strategy, particularly real‑world
evidence and post‑market commitments that increasingly influence regulatory and payer views, requires advance alignment. Leadership teams must decide upfront what evidence will matter, to whom, and when.
Financial and reputational exposure concentrates earlier across founders, investors, and leadership teams as consequential resource decisions must be made sooner in the development cycle. Previously, major capital commitments and leadership credibility were primarily at stake in late-stage development, after proof-of-concept was established. Now, defining strategic choices, such as manufacturing partnerships, pivotal trial design, and commercial preparation, must be made in early stages, when uncertainty remains high. Founder-led organizations face critical decisions sooner, often before governance structures fully mature. Capital decisions move forward as traditional stage boundaries blur, requiring upfront conviction with less downstream validation available.
Leadership expectations shift, as well. CEOs, CMOs, and senior R&D leaders must integrate scientific, regulatory, and commercialization judgment earlier in the lifecycle. Success depends on how effectively leadership teams align decisions, not just how quickly they move.
In this environment, compressed timelines reveal which organizations possess the leadership depth, decision discipline, and organizational readiness to act effectively under uncertainty. Speed amplifies existing capabilities — both strengths and weaknesses. Differences in governance, decision quality, and alignment become more visible and more consequential.
Boardroom Lens: Where Leadership Is Now Tested
For CEOs and boards, the implications move from concept to action. Faster pathways do not require new frameworks, but they do require different leadership behaviors. In a one‑pivotal‑trial environment, governance must support single‑shot execution. Engagement in trial design becomes unavoidable. Manufacturing and evidence strategies must keep pace with accelerated development.
Increasingly, this level of board engagement depends on having the right depth of scientific, regulatory, and operational expertise to make and govern high-stakes decisions effectively under uncertainty.
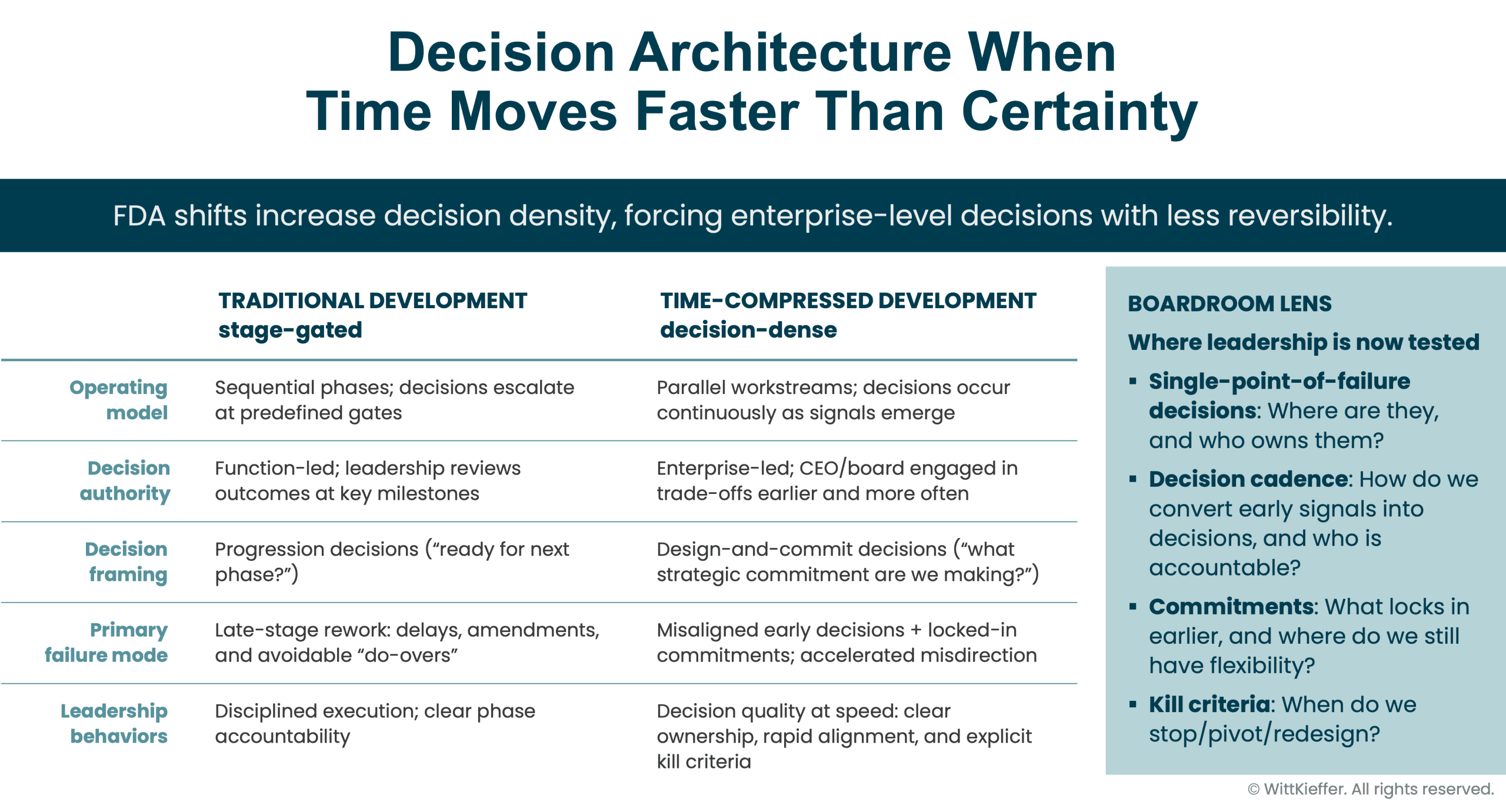
The challenge is practical and immediate. Leadership teams must address:
- Where are single‑point‑of‑failure decisions being made? Who owns them, and where are they concentrated: endpoint selection, patient population, comparator design, manufacturing path?
- How quickly can the organization convert early signals into decisions? What is the decision cadence, and who is accountable for interpreting, escalating, and acting as data emerge?
- Which commitments must be made earlier, and where has optionality already been lost, including manufacturing slots, CDMO selection, and evidence strategy? Where does flexibility remain?
- What kill criteria are in place, and is the organization prepared to use them? At what point should programs stop, pivot, or be redesigned if assumptions prove wrong?
Organizations that can answer these questions clearly — and operationalize the answers — are better positioned to benefit from accelerated learning. Those that cannot risk accelerating decision-making without improving decision quality first.
In this environment, size matters less than readiness. And leadership matters more than process.
About WittKieffer
WittKieffer is the premier executive search and leadership advisory firm developing impactful leadership teams for organizations that improve quality of life. We work exclusively with organizations in healthcare, science, and education — the Quality of Life Ecosystem — and provide essential knowledge, analysis, and perspective that produce effective leaders and inclusive cultures. Through our executive search, interim leadership, and leadership advisory solutions, we strengthen organizations that make the world better. WittKieffer is proud to be 100 percent employee-owned.











