The Physician Voice at the Table
Healthcare stands at an inflection point. The industry faces extraordinary pressures: rising costs that threaten organizational sustainability, quality imperatives that demand clinical excellence, regulatory complexity that requires sophisticated navigation, and a workforce crisis that challenges the very foundation of care delivery. In this environment, leadership models built for a more stable era are proving insufficient. Organizations that thrive are those that elevate physician leaders from bedside problem-solvers to enterprise architects, granting them genuine, cross-enterprise influence.
The business case for physician leadership has never been stronger. As healthcare organizations navigate the transition from volume to value, clinical decisions increasingly shape financial performance. A single protocol change can affect thousands of patients and millions of dollars. Technology investments in AI and clinical decision support systems require leaders who understand not only the promise of innovation, but its real-world impact on clinical workflows and patient outcomes. Population health initiatives demand expertise in care delivery models and the operational discipline to execute them at scale.
"A physician executive is, above all, a bridge builder: you have to understand both perspectives, speak both languages, and move fluidly between groups."
As a result, the physician executive role is expanding. Chief medical officers (CMOs), chief clinical officers (CCOs), and chief physician executives (CPEs) have traditionally been responsible for overseeing medical staff affairs, physician group practices, and core quality and safety functions. While these responsibilities remain foundational, they are no longer the primary source of impact for many organizations. Today, these leaders are members of the executive team who help set enterprise strategy, share accountability for financial outcomes, lead technology transformations, and reshape how care is delivered across inpatient, ambulatory, and virtual settings. Clinical credibility carries weight as a source of trust and legitimacy, but its power depends on how it is deployed. When a physician executive champions a new care pathway, it holds a unique resonance. These leaders speak the language of their physician colleagues, understand the nuances of patient care, and translate frontline realities into boardroom decisions, bridging the gap between strategic priorities and bedside execution.
What differentiates impactful physician executives, however, is not just the breadth of their remit, but their ability to lead through influence, aligning clinical, financial, and operational stakeholders in environments where authority is shared and formal control is limited.
"Physician executives now play a critical role in narrative storytelling — connecting clinical work to organizational goals for board and stakeholder engagement."
While CMO roles exist across diverse healthcare organizations, including biopharmaceutical companies, health plans, and digital health vendors, this research specifically focuses on health services organizations — hospitals, health systems, and academic medical centers — where clinical care delivery and operational complexity intersect most directly. The report below examines physician executive leadership through a combination of qualitative and quantitative research, drawing from in-depth interviews with sitting CMOs, CCOs, and CPEs, a survey of physician leaders, and an analysis of career pathways of physician executives at leading health systems.
The findings are clear: in today's healthcare landscape, physician leadership is foundational to performance; it is a critical organizational asset. Success requires moving beyond symbolic inclusion and instead placing physician leaders in roles of real influence — and understanding how that influence actually works.
Our Contributors
We are deeply grateful to the physician executives who generously shared their time, experiences, and insights for this research. Their candor and firsthand perspectives have been instrumental in illuminating the evolving landscape of physician leadership in healthcare.
Andy Anderson, M.D., Executive Vice President and Chief Medical and Quality Officer at RWJBarnabas Health
Theresa M. H. Brennan, M.D., Chief Medical Officer at University of Iowa Health Care Medical Center
Jonathan M. Buscaglia, M.D., Chief Medical Officer at Stony Brook University Hospital
Joseph C. Carmichael, M.D., Senior Vice President and Chief Medical Officer at UCI Health
Joseph M. Galante, M.D., Chief Medical Officer at UC Davis Medical Center
Chris A. Ghaemmaghami, M.D., Executive Vice President, Chief Physician Executive and Chief Clinical Officer at Jackson Health System
Caesar Gonzales II, M.D., Chief Clinical Officer at Trinity Health Michigan
Jamal Hakim, M.D., Chief Physician Officer at Orlando Health
Steven T. Hester, M.D., Senior Vice President and Chief Clinical and Strategy Officer at Norton Healthcare
Susan Huang, M.D., Chief Physician Executive at Providence
Gregory R. Johnson, M.D., Chief Medical Officer at UnityPoint Health
Kierstin Cates Kennedy, M.D., Chief Medical and Quality Officer at University Hospital, UAB Medicine
Sanjeeb Khatua, M.D., Chief Physician Executive at Endeavor Health
Ajay Kumar, M.D., Executive Vice President and Chief Clinical Officer at Hartford HealthCare
Adrian Moran, M.D., Chief Medical and Transformation Officer at MaineHealth
John D. Phipps, M.D., Executive Vice President and Chief Clinical Officer at UF Health
Andrew N. Pollak, M.D., Senior Vice President and Chief Clinical Officer at University of Maryland Medical System
Kevin Post, D.O., Chief Medical Officer at Avera Health
Iyad Sabbagh, M.D., Senior Vice President and Chief Physician Executive and President, Valley Physician Enterprise at Valley Health
Shlomit Schaal, M.D., Ph.D., Executive Vice President and Chief Physician Executive at Houston Methodist, President and Chief Executive Officer at Houston Methodist Physician Organization
Kevin R. Smith, M.D., Senior Vice President and Chief Medical Officer at Tucson Medical Center
Sowmya Viswanathan, M.D., Executive Vice President and Chief Physician Executive at BayCare Health System
Alon Z. Weizer, M.D., Senior Vice President and Chief Medical Officer at Mount Sinai Medical Center
Suzanne Wenderoth, M.D., former Executive Vice President and Chief Medical Officer at Tower Health
Managing Complexity: The Modern Physician Executive's Mandate
The physician executive role has undergone a fundamental transformation. What was once a position focused primarily on clinical quality and medical staff relations has evolved into a far more demanding leadership mandate — one that requires managing complexity across care delivery operations, financial stewardship, strategic planning, and enterprise-wide transformation. The data tells a compelling story: 81% of physician leaders report that their responsibilities have increased significantly or moderately over the past three years. This shift signals a redefinition of what physician leadership is expected to deliver in modern healthcare organizations.
The Physician Leadership Continuum
Physician executive roles span a continuum of increasing scope, authority, and enterprise impact. While titles such as CMO, CCO, and CPE are widely used, they are applied inconsistently and often interchangeably across organizations and do not reliably predict the substance of the role. In practice, physicians holding the same title may operate with radically different mandates, levels of authority, and strategic influence.
Rather than centering on titles, this research identifies three distinct physician leadership models, defined by scope of responsibility and where physician leadership is applied within the enterprise. These models coexist across health systems today, often simultaneously, and are shaped by organizational context, governance design, and strategic priorities. Organizations may deploy one, two, or all three models depending on their size, complexity, and stage of integration.
In the stewardship model, physician leadership is primarily oriented around safeguarding care standards and professional integrity. Leaders operating in this model focus on clinical quality and patient safety, medical staff affairs, regulatory compliance, accreditation, and physician engagement. Authority is typically concentrated within professional governance and quality frameworks rather than across operational or financial domains. This model is most common in organizations where physician leadership plays a critical role in maintaining care standards and clinician trust, while responsibility for operational execution and enterprise strategy resides with other executives.
Continuum in Physician Leadership Roles
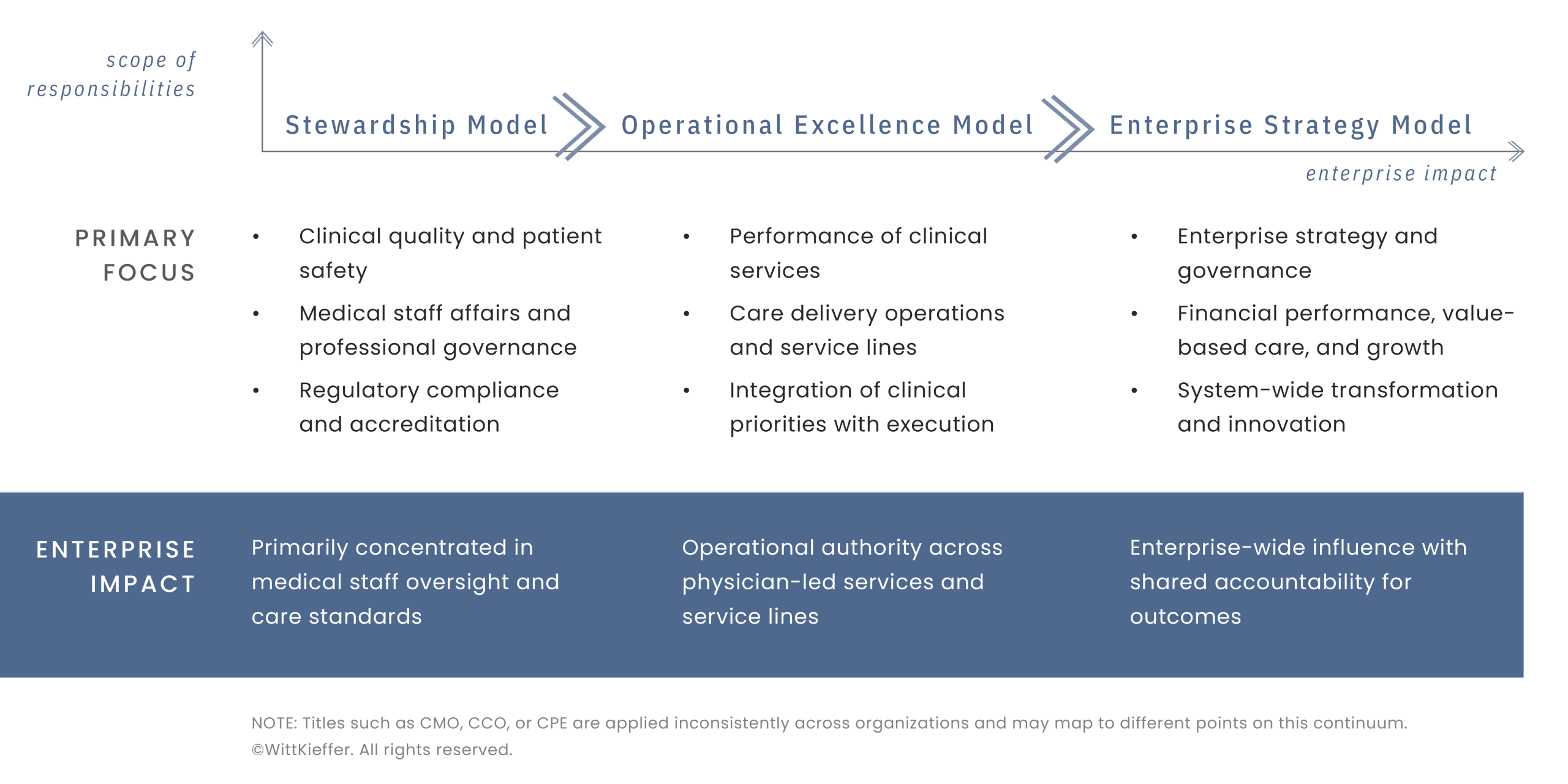
The operational excellence model reflects an expanded mandate in which physician leaders assume direct responsibility for the performance of clinical services and care delivery operations. In this model, physician leaders integrate clinical priorities with operational execution, exercise matrix authority across service lines or departments, and play a central role in care delivery redesign. Leaders operating in this scope often oversee service line performance, workforce deployment, throughput, and resource utilization, extending physician leadership beyond stewardship into day‑to‑day operating accountability.
"The right CMO for the right organization at the right time varies. You apply your core expertise where it matters most and develop a strong understanding in other areas while learning on the fly."
The enterprise strategy model represents the broadest scope of physician leadership, characterized by enterprise‑wide responsibility and strategic influence. Physician leaders in this model participate fully in C‑suite decision‑making, contribute directly to organizational strategy and governance, and share accountability for financial performance, growth, and transformation. These leaders integrate clinical, financial, and operational priorities, lead value‑based care and population health initiatives, and serve as enterprise architects for care delivery innovation. In this model, physician leadership is inseparable from business leadership. Clinical credibility serves as a source of legitimacy, but influence is exercised through strategic ownership and enterprise accountability rather than solely through professional authority.
Progression across these models is neither linear nor automatic. While organizations frequently deploy multiple models at the same or different points in their evolution, they often underestimate the intentional development required for leaders to operate effectively at broader scopes. A common failure is assuming physician leaders will naturally "grow into" expanded responsibility without structured development, deliberate coaching or mentorship, or a shared competency language to guide that transition.
"Sometimes we have to thread the needle to keep the hospital running successfully — and my goal as a CMO is ensuring quality, outcomes, and patients remain at the center of every decision."
At the organizational level, individual physicians may move between models over the course of their careers, and titles may remain static even as scope expands or contracts. In multi‑layered structures, clarity of decision rights and accountability becomes essential to avoid overlap, confusion, or gaps in leadership ownership. What matters most is not the title attached to a role, but the alignment between mandate, authority, and organizational need: ensuring the physician executive's authority, scope, and accountability are commensurate with the complexity of the mandate they are asked to carry out. Health systems in the midst of major integration efforts may require enterprise strategy leadership with system-wide authority. Organizations focused on operational performance and service line optimization may benefit from operational excellence leadership. Smaller systems or standalone hospitals may find the stewardship model sufficient. When physician leadership scope is well aligned with expectations, it creates momentum, supports sustained progress, and strengthens leadership impact at scale.
The Expanding Portfolio at the Intersection of Care, Cost, and Capacity
The physician executive role is a study in managed complexity. What was once a focused leadership remit is now a broad, interdependent portfolio that spans clinical, financial, technological, and human dimensions of the enterprise. Physician executives now carry responsibility across clinical quality, service line oversight, strategic planning, financial performance, technology enablement, and value-based care initiatives. This expansion in scope sets the context for a more consequential question: not whether physician executive responsibilities are growing, but how leaders are expected to deliver across an increasingly complex mandate.
Yet scope alone does not define the challenge. The more revealing insight emerges when examining how physician executives actually spend their time. Despite growing expectations around planning, innovation, and transformation, physician leaders remain heavily anchored in operational and administrative work, spending on average more than one‑fifth of their time (22%) on administrative and operational duties. What this reveals is a chronic altitude problem: physician executives are routinely pulled below the level of work their organizations say they need them to perform.
Importantly, this imbalance is not static. Leaders indicate an aspiration to shift time away from administrative and operational work and toward strategic leadership and innovation, yet structural barriers, including operational overload, insufficient infrastructure, unclear role expectations, and limited delegation, constrain their ability to do so. This is not simply a capacity issue. It reflects how roles are designed, what work is retained versus delegated, and whether organizations have built the management, analytic, and operational infrastructure that allows physician leaders to operate strategically.
When leaders remain persistently under‑altitude, the consequences extend beyond individual workload. Physician engagement suffers as leaders become less present and less credible as enterprise advocates, and strategic initiatives lose momentum as attention is diverted to near‑term operational issues. This imbalance exposes a persistent gap between organizational expectations and the practical realities of physician executive leadership.
Expanded Mandate of Physician Leaders
Beneath this expanding portfolio, four interdependent mandates are reshaping what physician executives are accountable for and the conditions under which they lead.
Financial stewardship has moved from peripheral awareness to core accountability. Physician executives are no longer expected simply to understand the financial implications of clinical decisions; many now carry direct responsibility for capital allocation, cost management, and clinical P&L performance. This evolution introduces continuous trade-offs between investment and sustainability. Seventy percent of survey respondents cite limited resources and budget constraints as their primary challenge, followed by navigating organizational politics as the second major challenge (46%), underscoring how financial pressure is frequently intertwined with governance and cultural complexity. While financial fluency has become table stakes, operating under financial constraint has emerged as a defining leadership condition.
Population health and care redesign denote another expanding area of accountability, one that demands sustained strategic focus. As organizations assume greater financial risk, physician executives are tasked with redesigning care pathways, managing clinical variation, and building proactive population health capabilities across inpatient, ambulatory, and virtual settings. This work requires systems-level thinking, longitudinal planning, and cross-functional coordination. Its impact is enterprise-wide, yet its execution is frequently slowed by the same capacity constraints affecting other enterprise priorities.
"My success in this role isn't about me — it's about others. It's about setting the tone and modeling expectations for hundreds of physicians, residents, and fellows. In enterprise leadership, the organization's story matters more than your own."
The physician workforce crisis is among the most urgent and emotionally charged mandates. Nearly half of physician executives identify managing physician burnout and well-being (46%) as well as physician recruitment and retention (40%) as top challenges. Leaders are navigating unprecedented levels of fatigue and disengagement while simultaneously asking clinicians to adapt to new technologies, performance expectations, and care models. This tension is compounded by role ambiguity and misaligned expectations, as physician executives are expected to be both organizational enforcers and physician advocates. Authentic engagement, trust, and credibility function as essential leadership currencies, requiring time, presence, and relational investment.
AI and clinical technology integration represents another critical mandate, and a major source of time tension. Physician executives are expected to lead the implementation of clinical decision support systems, AI-enabled diagnostics, and technology-enabled care delivery models. Yet the time allocation data suggests that the aspiration to lead innovation outpaces reality. While physician leaders aim to increase the time devoted to innovation and transformation, competing operational demands and insufficient infrastructure often keep many in a reactive posture. The challenge is not a lack of vision, but the structural difficulty of creating protected capacity to lead sustained change.
"As a physician executive, you should be a Swiss Army knife — able to move between clinical care, operations, finance, and business strategy. With the right skill set and portfolio, you become a critical organizational asset."
The cumulative effect is a role defined not by any single responsibility, but by constant prioritization under constraint. Physician executives must balance clinical excellence with financial performance, strategic ambition with operational reality, and physician engagement with enterprise accountability. The time allocation data underscores that many leaders are spending less time on the work their organizations increasingly value and more time navigating the friction between mandate and capacity.
Managing complexity and facilitating solutions, rather than mastering individual domains, is the defining work of modern physician leadership. Closing the gap between mandate and capacity requires not only expanded roles, but clearer expectations, stronger infrastructure, and leadership models that allow physician executives to operate less in firefighting mode and more in the strategic and transformational roles their organizations depend on.
The Leadership Journey: From Physician to Enterprise Leader
The journey from self‑managed clinician to enterprise‑level physician leader varies widely across individuals and contexts. Physician executives arrive at their roles through diverse trajectories shaped by organizational environment, institutional culture, developmental opportunities, and often, serendipity. What unites them is not a single prescribed pathway but rather a sequence of formative experiences that build the capabilities required to lead at scale.
"As a physician, I was trained to solve problems. Now, as a CMO, I diagnose and treat problems at a system level. The 'why' has always been making lives better; and now I'm doing it at scale for better outcomes for more people."
Understanding these journeys reveals both the evolution of physician leadership as a discipline and the persistent gaps between what medical education provides and what enterprise leadership demands. It also highlights the largely informal and uneven nature of physician executive development across health systems. This reality creates both opportunity and risk for organizations seeking to build sustainable leadership pipelines.
Pathways to the Top
While no two leadership journeys are identical, four distinct pathways consistently emerge from analysis of physician executives at the leading 200 health systems, reflecting ways clinical expertise translates into enterprise impact.
Clinical operations executive (40%). The traditional clinical ladder represents the most common route, progressing from clinician to medical director to vice president of medical affairs and CMO and, in some cases, to CPE. This pathway emphasizes incremental responsibility within clinical domains — leading a department, overseeing quality initiatives, managing medical staff relations — before expanding into broader operational and strategic roles. Leaders who follow this path often describe it as learning by doing, with each role building competencies required for the next. Because this progression is visible and well understood within most health systems, it remains the most reliable and readily identifiable pipeline for physician leadership development.
"Great sergeants don't always make good generals. The shift to physician executive leadership requires moving from hands-on daily operations to setting strategy and empowering others."
Clinical domain expert (30%). This route has traditionally moved from division chief or department chair to system‑level physician executive, particularly in academic medical centers where research, teaching, and clinical reputation confer administrative credibility. However, this path has become less linear and less sufficient over time, as chair and chief roles often lack sustained exposure to enterprise strategy, financial stewardship, and multi‑site operations. Increasingly, service line leadership serves as the critical bridge, providing accountability for financial outcomes, access and throughput, capital planning, workforce deployment, and operational performance across sites — experiences that more directly prepare physicians for executive physician roles.
Functional specialist (20%). This route reflects a newer pathway shaped by the growing importance of quality, informatics, and population health. Physicians with deep expertise in these domains, often holding roles like chief quality officer or chief medical information officer, transition into broader physician executive positions. This pathway produces leaders with sophisticated understanding of data analytics, process improvement, and technology-enabled care delivery. Their challenge is not credibility, but breadth: expanding beyond functional expertise to lead across the full spectrum of clinical operations and enterprise strategy. As AI integration, value-based care, and clinical digital transformation accelerate, this pathway is becoming increasingly prominent.
Strategic operator (10%). The operational hybrid pathway represents a less common route, where physician executives move laterally into operational roles, serving for a certain period of time as as CEOs, regional presidents, or chief operating officers, before returning to system-level physician executive positions. This pathway produces leaders with comprehensive understanding of healthcare operations, financial management, and enterprise strategy. They bring credibility not only as clinicians but as operators who have managed budgets, led turnarounds, and driven organizational performance.
These pathways are not mutually exclusive. Many physician executives describe hybrid journeys that combine elements of multiple routes. What matters is not the specific path but whether the journey provides exposure to clinical operations, financial stewardship, strategic planning, and organizational leadership — the core domains that define modern physician executive work.
The profile of today's physician executive reinforces the absence of a single leadership archetype. As shown in the accompanying portrait of physician leaders across leading health systems, physician executives vary widely in demographics, role tenure, specialty background, and professional preparation, reflecting multiple points of entry into enterprise leadership rather than a uniform progression.
Physician Leadership at Health Systems: A 2026 Portrait
Demographics
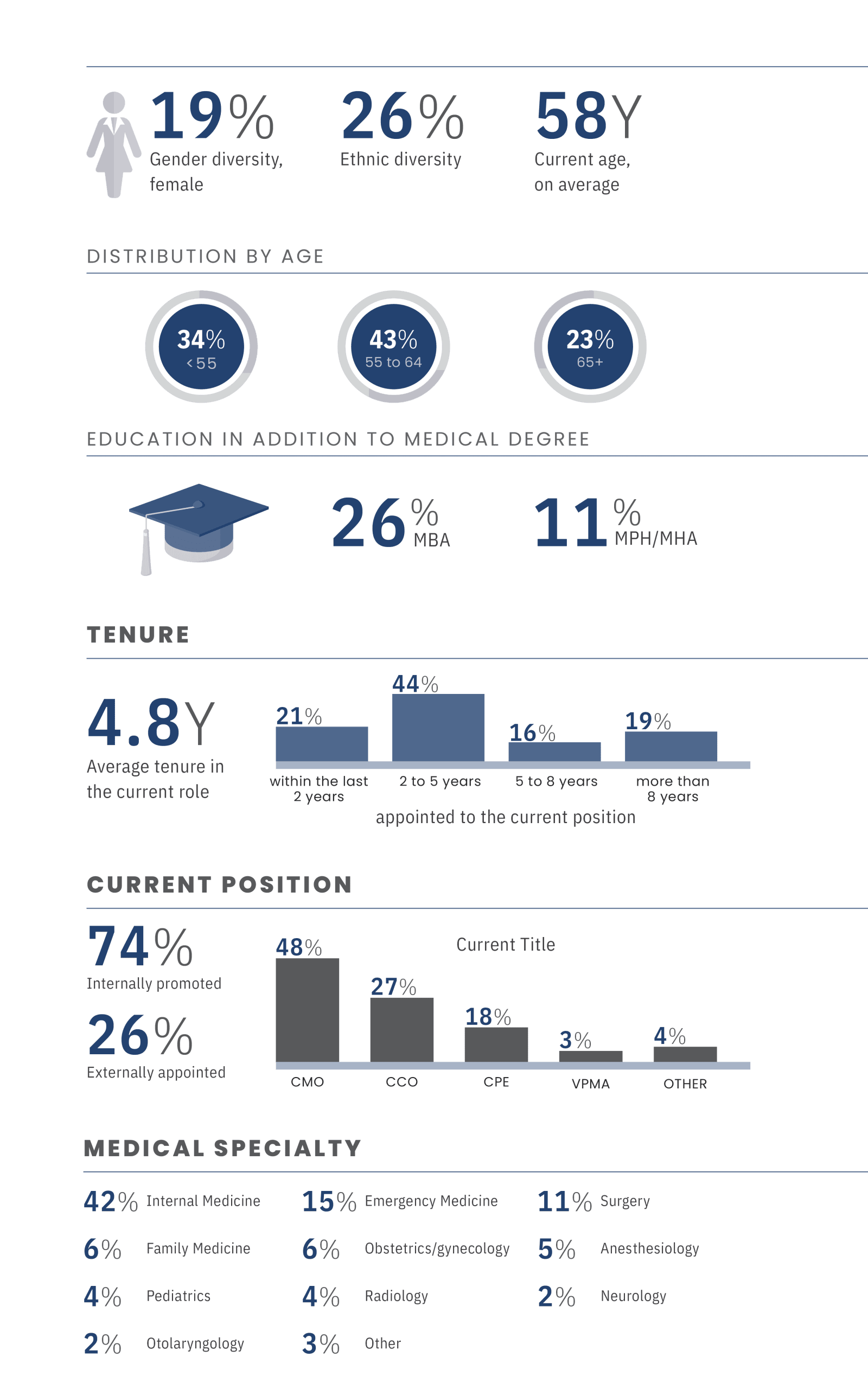
Clinical backgrounds among physician executives are heterogeneous. No single specialty dominates the leadership ranks, with representation spanning internal medicine, emergency medicine, surgery, family medicine, and a broad range of other disciplines. This dispersion reinforces a consistent theme that success as a physician executive depends far less on clinical specialty than on the ability to lead across disciplines, navigate complexity, and integrate clinical and business priorities.
"An enterprise physician leader must let go of the idea that this work is about you or your specialty. It is about leading medicine at scale, serving not only patients, but also physicians, teams, and the systems that shape care for many. That shift in mindset is not easy. For surgeons, it often means stepping away from the operating room and the privilege of caring for one patient at a time. It is one of the hardest sacrifices we make. But in return, you gain the opportunity to improve care for countless patients and to elevate the experience of those who deliver it. This work asks you to stay humble, to remain a continuous learner, and to find purpose in impact beyond yourself."
Educational preparation further illustrates the diversity of leadership formation. More than a quarter of physician executives hold MBA degrees, and many others have earned MPH or MHA credentials, reflecting growing recognition of the need for financial, operational, and strategic fluency beyond medical training. At the same time, these credentials are not universal, underscoring that many leaders develop enterprise capabilities through experience rather than formal education.
Combined, the profile highlights why multiple leadership pathways persist. Differences in background, preparation, and opportunity shape how physicians enter and advance into executive roles.
Where Medical Training Ends — and Executive Leadership Begins
The transition from clinician to enterprise leader exposes significant gaps between medical training and the competencies required for physician executive effectiveness. Medical education is designed to prepare physicians to diagnose and treat individual patients, not to lead organizations, manage budgets, or drive system-wide change. As physicians move into executive roles, these gaps become increasingly visible and consequential.
"Careers grow on saying yes. Leadership begins when saying no becomes necessary — and that pivot is genuinely hard."
The skills medical training does not emphasize are precisely those that define physician executive work. Financial literacy, covering understanding P&L statements, capital allocation, and return on investment are rarely part of formal medical education, yet they become essential for physician executives responsible for clinical operations and enterprise-level resource decisions. Strategic planning, organizational design, and change management are similarly absent from traditional curricula. Clinical training develops rigorous problem-solving capabilities but it does not equip physicians to lead teams at scale, influence across reporting lines, or navigate the political dynamics of matrixed organizations.
The transition from clinical practice to administrative leadership also requires fundamental shifts in mindset and approach. Physicians are trained to be autonomous decision-makers, while physician executives must lead through collaboration, alignment, and influence. Clinical practice rewards individual expertise and direct intervention; executive leadership depends on building systems, empowering others, and accepting indirect control and delegation. Medicine favors evidence-based decisions with clear right answers; organizational leadership is shaped by ambiguity, trade-offs, and decisions made with incomplete information. This shift from individual authority to distributed leadership is among the most difficult adjustments physicians face when entering executive roles.
"Know thyself. Leadership starts the same way medicine does: by understanding the whole person — you. Tools and training help build new skills, but without self-awareness, you risk losing your mojo — the natural strengths that made people want to follow you in the first place."
Less visible, but equally consequential, is the self‑management dimension of this transition. Impactful physician leadership begins with self‑awareness: understanding how one's professional formation, leadership instincts, and sources of authority shape behavior at scale. Many physician executives describe an inflection point where clinical identity, once a source of strength, must be consciously recalibrated to remain effective at the enterprise level. In practice, limitations in self‑awareness — not gaps in strategic or financial knowledge — often become the rate‑limiting factor in leadership development. Sustained effectiveness depends on the ability to release individual control, reorient purpose from personal clinical impact to system‑level influence, and lead with emotional intelligence as responsibility expands.
Role Preparation
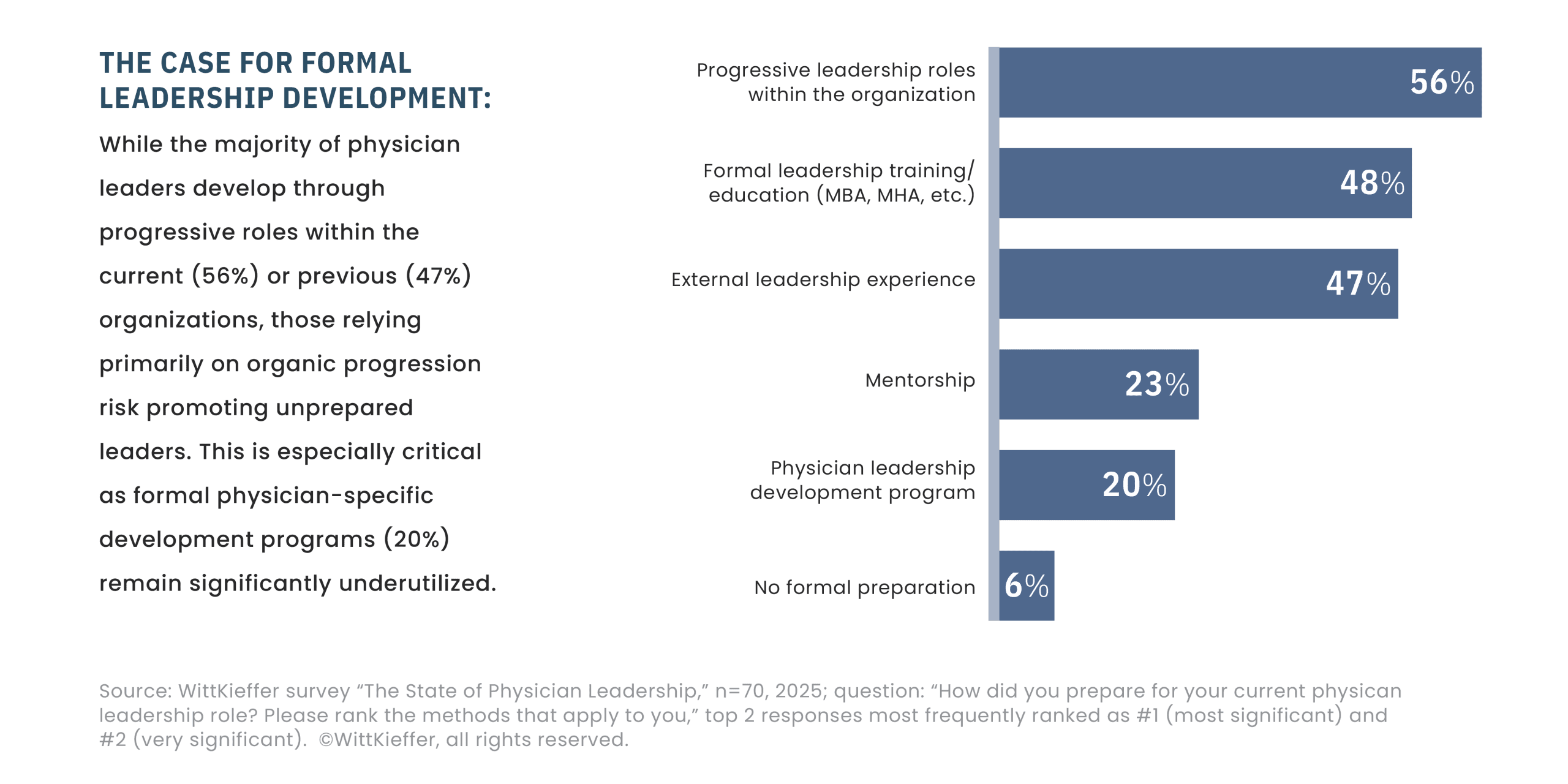
Development experiences that support this transition tend to follow consistent patterns. Formal leadership development programs provide foundational exposure to finance, strategy, and organizational behavior, creating a shared vocabulary for enterprise leadership. However, physician‑specific leadership development remains notably underutilized, with only 20% of physician executives reporting participation — a finding that highlights a central structural gap rather than a marginal one.
At the same time, more general business and health administration education, including MBA, MPH, or MHA programs, plays a more prominent role in preparation, reflecting efforts to supplement medical training rather than replace experiential learning. While these programs build important technical fluency, they are not designed for the specific context of physician executive leadership, such as leading through professional authority, shared governance, clinical credibility, and mission‑driven cultures while carrying enterprise accountability.
"Clinical practice, especially in the emergency department, builds emotional intelligence. It teaches you how to read situations and people quickly — and how not to create chaos. These skills carry straight into leadership: bringing calm, asking the right questions, and solving the problem in front of you."
What the data ultimately reveal is that most physician executives develop enterprise leadership capability primarily through exposure and trial, rather than through deliberate, competency‑grounded programs tailored to physician leadership. The most consequential learning occurs through experiential development: leading a quality or transformation initiative, managing a service line, participating in executive decision-making, or taking responsibility for outcomes beyond a single department. Consistent with the survey findings, these experiences most often occur through progressive leadership roles within the physician's current organization (56%) or a previous organization (47%). Operating in these roles forces physicians to step outside the clinical frame and engage directly with the realities of organizational complexity.
Exposure to diverse organizational functions further differentiates physician executives from department-level leaders. Time spent working alongside finance, operations, strategy, or technology teams builds fluency in how decisions are made, constraints are managed, and priorities are negotiated across the enterprise. This cross-functional exposure is central to developing an enterprise mindset — one that extends beyond clinical excellence to organizational performance, sustainability, and scale.
Mentorship and sponsorship play a critical role in accelerating this development. Nearly one quarter of physician executives (23%) identify mentorship as a significant contributor to their leadership preparation, reflecting the importance of relationships that provide guidance, perspective, and access to expanded responsibility. Where mentorship is intentional and supported, enterprise perspective develops earlier and more consistently; where it is informal or absent, readiness varies widely.
"We assume physicians know how to lead, but leadership isn't innate — it's a skill, and like any other skill, it must be honed over time. Today's expectations leave little room to learn it on the job; physician executives must arrive with a baseline leadership skill set: self-management, ability to navigate difficult conversations, and emotional intelligence.”
Taken together, these gaps and experiences illustrate a structural reality: physician executives are often asked to operate at an enterprise level before they are systematically prepared to do so. The development gap represents both a challenge and an opportunity. Organizations that rely on ad hoc learning and assume clinical excellence will translate into leadership capability face persistent variability in executive effectiveness. Those that recognize physician executive leadership as a distinct discipline — and invest in development accordingly — are better positioned to build durable leadership capacity and a deeper bench of future enterprise leaders.
The majority of physician executives leading today's health systems followed varied and often unstructured development pathways. They navigated ambiguous transitions, acquired critical skills on the job, and adapted their leadership approach through experience rather than formal preparation. The question for healthcare organizations is no longer whether these gaps exist, but whether they will continue to rely on individual resilience — or intentionally build the infrastructure, programs, and self-reflection mechanisms required to systematically prepare physicians for enterprise leadership.
The Art of Influence: How Physician Leaders Drive Change
Physician executives operate at the center of modern healthcare organizations — but rarely at the center of authority. They work within matrixed organizations where decision rights are shared, accountability is diffuse, and outcomes depend on alignment across clinical, financial, and operational domains. In this environment, effectiveness is not determined by title or positional power. It is determined by influence: the ability to shape decisions, mobilize stakeholders, and move complex systems forward without direct control.
Influence, however, is often misunderstood. It is not a soft skill layered onto "real" leadership, nor a substitute for authority. For physician executives, influence is the primary operating system of leadership. Understanding how it works, and where it breaks down, is essential to understanding how change actually happens in healthcare organizations.
Influence as the Operating System
Physician executives do not lead through command-and-control structures. Authority is diffuse by design: service lines cut across hospitals, physicians report through multiple lines, and enterprise decisions require alignment among peers with competing priorities. In this context, influence is not a leadership style choice; it is the only scalable mechanism available. At the same time, influence is not solely an individual capability. It is also a system property, shaped by role design, decision rights, governance clarity, and how accountability is structured across the organization.
Effective influence is built early, not deployed late. It is established through sustained engagement, clarity of intent, and a track record of follow‑through before decisions are formally on the table. When physician executives are forced to escalate or "pull rank,"it is rarely a success. It usually signals that alignment failed upstream.
Influence does not eliminate conflict. It creates the conditions to surface it productively: shaping how decisions are framed, who is involved, and how trade‑offs are owned. That work, more than authority alone, determines whether change actually sticks.
"If you have to pull the authority card, consider it a failure. Real leadership happens through influence. If you're relying on authority, you probably missed the opportunity to lead through influence earlier."
Clinical Credibility Has Limits
Clinical credibility remains essential to physician leadership because it establishes legitimacy with clinicians and signals proximity to patient care. Yet on its own, it rarely moves enterprise decisions forward. In executive settings governed by trade‑offs rather than absolutes, credibility must be translated to remain influential.
"Having an open mindset is critical — being willing to listen, adapt, and adjust. Optimism matters a great deal, because once you go negative, it doesn't help you or anyone around you. The positive energy you bring as a leader carries through the entire organization."
What resonates with physicians (clinical evidence, professional norms, patient impact) often fails to persuade peers in finance, operations, or strategy unless it is reframed in economic, operational, or risk‑based terms. Influence increases not when clinical credibility is asserted, but when it is integrated into enterprise decision logic.
"For aspiring CMOs, one of the most important realizations is that you belong at the executive table. Sitting alongside the COO, CFO, and others can feel intimidating, but you're there because you bring equal expertise. The role requires embracing that responsibility — being a strong advocate for the clinical perspective while keeping the broader organizational picture in mind."
Over‑reliance on the physician voice can, paradoxically, weaken influence. When clinical credibility is used to resist constraints rather than engage them, it is perceived as partial advocacy rather than leadership. The most effective physician executives treat credibility as an entry point, never a conclusion, using it to bridge domains and connect clinical insight to system performance and sustainability.
From Advisor to Owner
Sitting at the executive table now carries an expectation of shared accountability for enterprise outcomes, not just representation of clinical interests. Influence with peers depends less on expertise than on demonstrated willingness to absorb risk and own trade‑offs alongside other executives.
"Physicians carry their comfort with uncertainty into the C-suite. Their willingness to declare what they don't know and embrace the unknown is a leadership asset."
This shift demands comfort with uncertainty. Executive decisions are often made with incomplete information, competing imperatives, and imperfect options. Physician leaders who insist on clinical certainty can stall progress; those who acknowledge ambiguity and help frame viable paths forward gain influence. In this context, declaring what is not yet known is not a weakness; it signals maturity and trustworthiness.
Influence grows when physician executives are seen not as translators of clinical opinion, but as enterprise leaders capable of integrating clinical, financial, and operational realities into coherent direction.
Influence with Physicians
Influence with physicians is both foundational and fragile. It is slow to build, quick to erode, and difficult to repair once lost. Unlike C‑suite peers, physicians experience the downstream effects of executive decisions directly, making perceived inconsistency or opacity especially damaging to trust.
"The fundamentals will always matter: being a good communicator and a good listener. This is especially true in healthcare. With so many competing priorities, you have to make a compelling case for direction and get people to follow you."
Clinical presence matters, but proximity alone does not sustain influence. Credibility is reinforced through predictability, transparency, and follow‑through: clear explanations of why decisions are made, what trade‑offs were considered, and how concerns will be addressed over time. Symbolic leadership fails fastest with physicians, who readily distinguish between engagement and performance.
Impactful physician executives function as translators and boundary‑holders, articulating constraints honestly while maintaining visible commitment to professional values and patient care. In this arena, influence is less about persuasion and more about trust built through consistency under pressure. Importantly, the connecting role of physician leaders is also seen as a marker of organizational health and culture.
"Words matter in leadership — they shape strategy and inspire teams. Choose them carefully, because what you say carries weight that extends far beyond the conversation."
Productive Disagreement
High‑performing physician leadership does not depend on consensus. It depends on productive disagreement. In complex health systems, the absence of tension is rarely a sign of alignment; it is more often a signal that dissent has gone underground.
Effective dyad and triad models normalize debate as part of decision‑making. Influence is exercised by creating environments where disagreement is safe, roles are clear, and conflict is surfaced early, before positions harden or workarounds emerge. Suppressing friction in the name of harmony slows execution and weakens accountability.
Impactful physician executives design for debate, clarify decision rights, and ensure that disagreement informs — not derails — progress. When treated as a design feature rather than a leadership failure, disagreement allows influence to scale.
"Disagreement is foundational to the dyad model. Debate drives better outcomes — but only if you build a culture where that debate is truly acceptable."
Influence is not infinitely elastic, and even exceptional physician leaders cannot compensate indefinitely for poor organizational design. When physician executives repeatedly struggle to move decisions forward, the problem is rarely skill, effort, or intent. More often, it reflects misalignment between expectations and authority, scope and infrastructure.
Organizations that depend on influence to overcome unclear governance or under‑designed roles eventually exhaust their leaders. Escalation increases, trust erodes, and leadership turnover accelerates — not because physician executives lack capability, but because influence is being used as a substitute for structure.
The art of influence, then, is not merely a personal attribute. It is a diagnostic lens on organizational design. Where influence works, structures, decision rights, and incentives are aligned. Where it consistently fails, the system is revealing its limits. The central question is not only whether physician executives can lead through influence, but whether organizations are willing to design environments where influence can translate into durable, scalable impact.
The Road Ahead: Leading in the Next Era
"My advice to physicians who want to move into leadership: join a committee, volunteer, raise your hand. Start somewhere with intention, because those experiences are how you learn, build credibility, and get asked to lead."
The physician executive role will continue to evolve, shaped by technological disruption, sustained financial pressure, and fundamental changes in how healthcare is delivered and financed. The question facing organizations is no longer whether physicians belong in enterprise leadership roles, but whether those roles are designed — and leaders prepared — for what comes next. The next era will magnify both the opportunity and the challenge of physician leadership.
Foundational leadership capabilities such as communication, change management, and strategic thinking remain essential. They are the table stakes of modern healthcare leadership and closely tied to the influence‑based models that define physician executive work today.
"Future physician executives must be attuned to both the cost side of the equation and the cultural dynamics of their organizations — understanding their executive peers' challenges while building collaborative support."
Yet the future demands a materially expanded skill set. As organizations adopt advanced analytics, AI‑enabled decision support, and increasingly elaborated digital platforms, physician executives must lead not only through change but through sustained technological transformation. This shift is sharp and unmistakable: while just 8% of physician executives identify AI and machine learning expertise as critical today, 41% view it as essential for future success, signaling a decisive inflection point in leadership expectations.
Technology fluency is rapidly becoming a core leadership competence. This does not require physician executives to become technologists, but it does require literacy: understanding how technology is applied in clinical settings, evaluating data validity and algorithmic bias, and ensuring that digital tools improve rather than complicate clinical workflows. Leading technology adoption is as much about trust, workflow redesign, and clinical engagement as it is about systems and software. Similarly, the proportion of leaders identifying technology and digital health experience as critical rises from 8% today to 24% looking ahead, underscoring that digital acumen is moving from specialized expertise to executive baseline.
"Physician leaders must embrace technology and help others through it — to be change champions. And flexibility is just as critical. Change is happening so rapidly that we can't be reactive to the point where it cripples us. We have to anticipate what's coming and be ready to pivot quickly."
At the same time, the increasing pace of transformation raises the bar for judgment. Advanced tools amplify — not replace — the need for discernment, prioritization, and human connection. Physician executives must hold multiple tensions simultaneously: speed and patience, innovation and stability, performance and trust. The physician executive role is often one of constant translation between two worlds: the clinical realm, requiring the swift, tactical agility of a fighter pilot, and the administrative realm, demanding the strategic patience of an aircraft carrier captain.
Throughout this transformation, the core purpose of healthcare must remain intact. Influence in the next era will not be sustained by technical expertise alone, but by leaders who retain credibility with clinicians and keep patients at the center of decision‑making, even as systems grow more complex and data‑driven.
"Future leaders must hold many skills and competencies — but never lose sight of the core: healthcare is one human being coming alongside another in their suffering. We care for neighbors, not just customers."
Importantly, these capabilities do not emerge by accident. Effective physician leadership is built through exposure, intentional assignments that push leaders beyond familiar territory, and accumulation of responsibility over time. Leadership readiness develops not only through formal education, but through early opportunities to lead, to fail, and to learn.
The road ahead, therefore, demands more than individual adaptability. It requires organizational intention. Physician executives succeed not because they are persuasive, but because they operate in environments where influence can take hold and where roles are clear, debate is safe, and accountability is shared.
Healthcare organizations now face a defining choice. Those investing deliberately in developing clinically credible, technologically fluent, enterprise‑minded physician leaders will build the leadership capacity required for the next era. Those assuming clinical excellence will naturally translate into enterprise leadership will continue to experience gaps between the leaders they need and the leaders they have.
About WittKieffer
WittKieffer is the premier executive search and leadership advisory firm developing impactful leadership teams for organizations that improve quality of life. We work exclusively across healthcare, science, and education, providing essential knowledge, analysis, and perspective that produce effective leaders and inclusive cultures.
WittKieffer’s Physician Leadership Institute
The Physician Leadership Institute equips physicians with the skills and insights needed to excel in leadership roles, ultimately driving positive change and organizations. Through individual and growth to build sustainable healthcare cohort training, the Physician Leadership Institute helps participating physician leaders deepen their awareness of their own needs and provides them with the tools to meaningfully advance as leaders.









